
Debunked: This misleading NYT anti-trans column relies on pseudoscience
by Curated February 3, 2024 · Gay News / Gay Pride / Gay Rights / The Advocate
Author: Erin Reed
In an article published in the opinion section of The New York Times, opinion columnist Pamela Paul wrote a 4,500-word article filled with factual errors and unfounded assumptions about transgender care and the lived experiences of transgender people. Although the article is presented as a piece on detransitioners, the interviews serve as vehicles through which Paul packages inaccuracies and disinformation with faulty citations and claims that are not supported by the evidence she presents. The article is the latest in a series published by The New York Times to do so, and a simple fact check of the claims presented easily debunks the article’s central premises as highly misleading.
Claim: In April 2022, the Oregon Board of Licensed Professional Counselors and Therapists told Winn that she was under investigation. Her case was ultimately dismissed, but Winn no longer treats minors and practices only online, where many of her patients are worried parents of trans-identifying children.”
“So Your Kid Wants To Live As The Opposite Sex” by Stephanie WinnStephanie Winn has not been investigated or attacked simply for “approaching gender dysphoria in a more considered way.” Rather, attacks on Winn are linked to extremely cruel suggestions and musings around how transgender youth should be dealt using cruel, coercive, and painful conversion therapy techniques.
Claim: …
“I transitioned because I didn’t want to be gay,” Kasey Emerick, a 23-year-old woman and detransitioner from Pennsylvania, told me. Raised in a conservative Christian church, she said, “I believed homosexuality was a sin.”
Studies show that around eight in 10 cases of childhood gender dysphoria resolve themselves by puberty and 30 percent of people on hormone therapy discontinue its use within four years, though the effects, including infertility, are often irreversible.
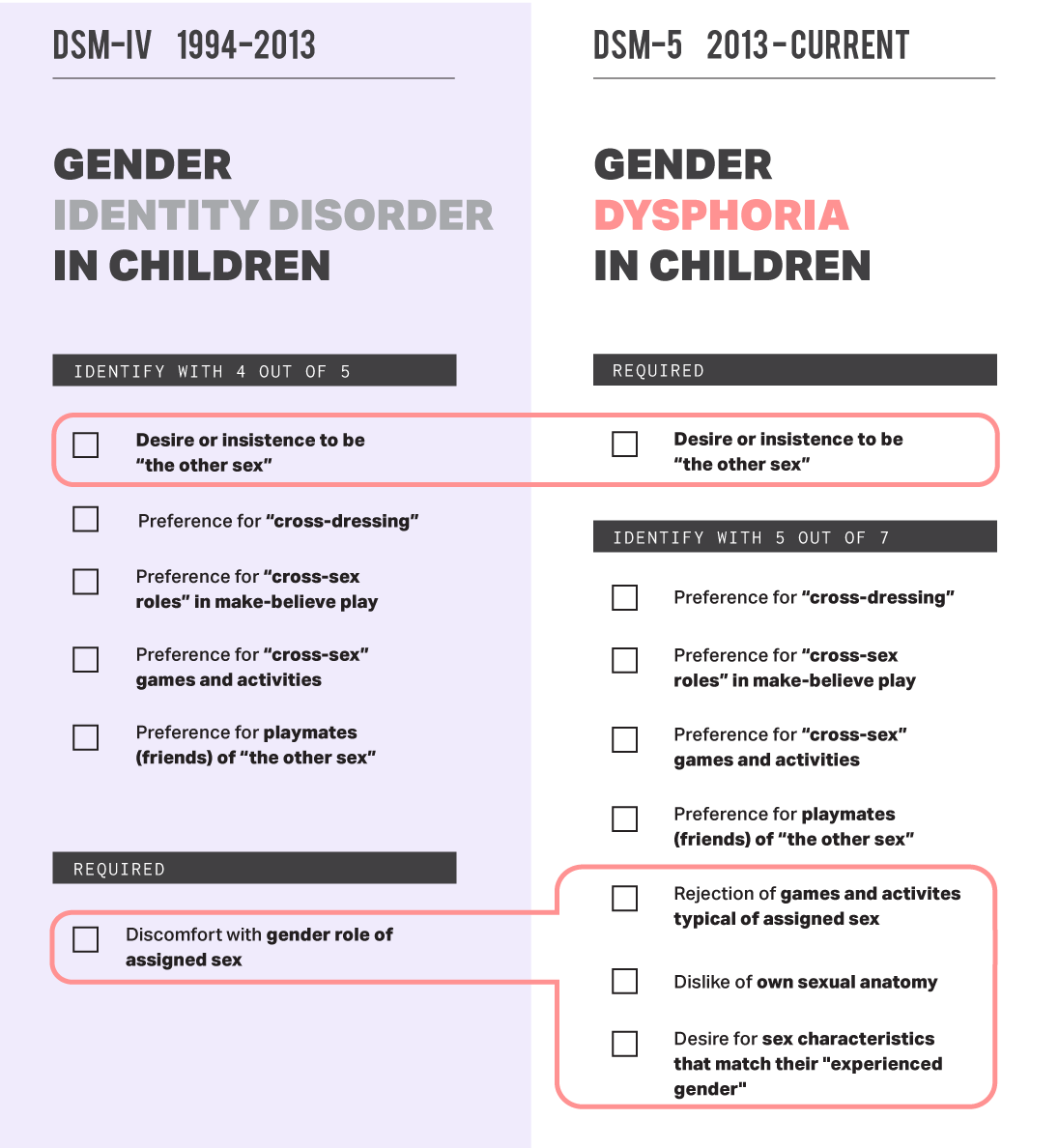
Old criteria vs. new criteriaSteensma’s2011 and 2013 studies had similar issues in his research, which in some ways had even worse methodological flaws. Steensma used the old criteria, which is not the way that gender dysphoria is diagnosed today. Worse, the two studies classified every youth who did not return to the clinic as having “desisted” or “detransitioned” with no long term follow-up. Half of the participants in the studies did not return and all were classified as having “desisted.” The sample sizes were tiny at the getgo – only 53 people were in the first study and 127 in the second study. Given the fact that a large portion if not the majority of Steensma’s patients were classified under decades old criteria and assumed permanently detransitioned simply for refusing to follow up, these studies cannot be used to make any reasonable claim of high desistance rates.
The last study that Paul refers to is a study released two years ago on military continuance of care. That study looked at all hormone therapy distributed under the military Tricare health insurance plan and determined that 30% of people stopped receiving their hormones through Tricare. What the study does not do, as Paul claims, is support the idea that “30% of people discontinued hormone therapy.” In fact, there are many reasons why people would no longer fill their hormone therapy through a military Tricare plan, especially towards the end of the study in 2017-2018:
- The Trump administration began targeting transgender servicemembers, and many transgender servicemembers likely stopped filling their hormone prescriptions through Tricare for themselves or their family members, fearing being targeted.
- Tricare has notoriously poor transgender care coverage, as evidenced by many military members responding to a thread discussing the results of this study, and many transgender servicemembers may opt to get their medication through a low cost alternative such as Planned Parenthood
- Hormone therapy can be discontinued for surgery, fertility and pregnancy planning, and many other purposes.
- Some nonbinary patients may obtain all the results they wish from hormone therapy before discontinuing, desiring no future results.
- Transgender people may simply have not filled the medication through insurance and instead utilized online pharmacies, which have grown increasingly popular.
- Transgender patients can easily fill prescriptions through GoodRX plans, which would allow them more privacy.
- Transgender people may have been forced off care by military decisions
Even the authors of the article themselves state that they likely overestimate discontinuation:
“We only collected information on medication refills obtained using a single insurance plan. If patients elected to pay out of pocket for hormones, accessed hormones through nonmedical channels, or used a different insurance plan to pay for treatment before and/or after obtaining gender-affirming hormones using TRICARE insurance, we did not capture this information. This means that our findings are likely an underestimate continuation rates among transgender patients.”
There are many more factual errors contained within Paul’s article; it is 4,500 words long and covers virtually every anti-trans claim made in legislative hearings across the United States. Many advocates for transgender people, medical experts, and journalists have weighed in to cover other aspects of Paul’s piece. You can find those here:
From Your Site Articles
Original Article on The Advocate
Author: Erin Reed

